mpfl Reconstruction
What is the Medial Patellofemoral Ligament (MPFL)?
The MPFL, or medial patellofemoral ligament, is a strong band of connective tissue on the inner side of the knee. Its main job is to keep the kneecap (patella) stable as the knee bends and straightens. The patella naturally moves up and down within a small groove at the front of the thigh bone (femur). The MPFL acts like a soft-tissue safety strap that prevents the kneecap from sliding sideways to the outer part of the knee.

What is MPFL Reconstruction?
MPFL reconstruction is a surgical procedure that restores stability to the kneecap (patella) when it has been damaged or stretched due to repeated dislocations. The medial patellofemoral ligament (MPFL) is a key soft-tissue structure on the inner side of the knee. It acts like a restraint that keeps the kneecap from sliding sideways. When this ligament tears, the patella can become unstable and prone to slipping out of place, leading to pain, swelling, and reduced confidence when walking or playing sports.
Reconstruction involves creating a new ligament using a small tendon graft, which is anchored to the patella and the femur to replicate the MPFL's natural function. Modern techniques keep the procedure minimally invasive, preserve healthy tissue, and allow for a gradual return to normal activities.

Who is Suitable for MPFL Reconstruction?
This procedure is generally recommended for people who experience ongoing kneecap instability that does not improve with physiotherapy and other conservative treatments. Suitability is based on a combination of symptoms, structural findings, and activity goals.
Common groups who may benefit include:
- Patients with recurrent patellar dislocations: Those who have dislocated their kneecap more than once often have MPFL damage that no longer heals on its own.
- Individuals with persistent instability: Even without a full dislocation, some patients feel the kneecap “slip,” especially when turning, kneeling, or walking downhill.
- Active patients: Athletes or those involved in physically demanding work may require a stable knee to safely perform their activities.
- People with MPFL tears confirmed by imaging: MRI scans often show a stretched or ruptured ligament that contributes to instability.
- Those without severe bone alignment issues: MPFL reconstruction works best when bony anatomy is normal or only mildly altered. In complex cases, additional procedures may be needed.
Benefits of MPFL Reconstruction
MPFL reconstruction aims to stabilise the kneecap and improve the quality of life. Many patients notice immediate improvements in confidence and function as healing progresses.
Key benefits include:
- Improved patellar stability: The reconstructed ligament helps prevent further dislocations and reduces the feeling of the knee giving way.
- Reduced pain and swelling: Recurrent instability often causes irritation and cartilage stress; stabilising the patella helps relieve these symptoms.
- Better knee function: Patients can return to walking, sports, and daily tasks with greater ease.
- Protection of knee cartilage: Fewer dislocations reduce the risk of long-term joint damage and early arthritis.
- Minimal cosmetic impact: Modern techniques use small incisions.
- Reliable outcomes: Success rates are high when the surgery is paired with a structured rehabilitation program.
Types of MPFL Reconstruction
There are several approaches to MPFL reconstruction, and the choice depends on the anatomy, age, prior injuries, and the surgeon's preference. All types aim to restore the ligament's natural tension while avoiding excessive force on the patella.
Common types include:
- Autograft MPFL reconstruction: This uses the patient’s own tendon, often the hamstring (gracilis or semitendinosus). It is the most common method because it integrates well with the body and carries a low risk of rejection.
- Allograft MPFL reconstruction: This uses donor tissue. It is a good choice for patients who prefer to avoid tendon harvesting or who have already used their hamstring tendons in previous surgeries.
- Suture-tape or synthetic augmentation: A reinforced synthetic material is used to support or replace the ligament. This technique can be useful in selected cases, especially when rapid early stability is beneficial.
- Anatomic double-bundle reconstruction: This technique recreates the two functional bundles of the MPFL to more closely mimic natural ligament behaviour. It may offer improved rotational control of the patella.
- Paediatric MPFL reconstruction: Special approaches are used in children and adolescents to protect growth plates while rebuilding stability.
Surgeons choose the method that best suits the patient’s anatomy, activity level, and goals.
Alternative Options to MPFL Reconstruction
Not all patients require surgery. Many benefit from non-invasive or less complex treatments, especially after a first-time dislocation or when instability is mild.
Useful alternatives include:
- Physiotherapy: Strengthening the quadriceps (especially the vastus medialis), improving hip and core strength, and correcting movement patterns can help stabilise the kneecap. This is often the first line of treatment.
- Bracing: A patellar-stabilising brace can be worn during sport or high-risk activities to reduce the chance of the knee giving way.
- Activity modification: Avoiding deep squatting, sudden twisting, or uneven surfaces can reduce strain on the knee while it heals.
- Taping techniques: Kinesiology taping or rigid taping can support patellar tracking during rehabilitation.
- Pain-relief medications and anti-inflammatory treatment: Used to manage symptoms and allow more comfortable exercise.
- Weight management: Reducing excess load can protect the knee joint and relieve discomfort.
- Corrective surgery for underlying causes: In some cases, bone alignment issues such as trochlear dysplasia, patella alta, or tight lateral structures may be the primary issue. Procedures like tibial tubercle osteotomy, trochleoplasty, or lateral release may be considered with or instead of MPFL reconstruction.
Preparation Before an MPFL Reconstruction
Preparing properly for MPFL reconstruction helps ensure a smooth procedure and a more comfortable recovery. Before surgery, your surgeon will complete a detailed assessment, review your imaging, and confirm that surgery is the best option for your knee. You may also work with a physiotherapist to strengthen your muscles beforehand, as this can speed up rehabilitation.
Patients are usually advised to:
- Attend a pre-operative assessment: This includes a clinical examination, review of X-rays or MRI scans, and discussion about the surgical plan.
- Complete pre-habilitation exercises: Strengthening the quadriceps, hamstrings, hips, and core improves early recovery, reduces swelling, and assists with walking after the procedure.
- Adjust medications if needed: Your doctor may advise stopping certain blood-thinning or anti-inflammatory medications before surgery.
- Organise home support: Arrange help with transport, household tasks, or work adjustments during the first few days after surgery.
- Prepare mobility aids: Items such as crutches, ice packs, or raised seating can make the early recovery period easier.
- Follow fasting instructions: Patients are guided on when to stop eating or drinking before anaesthesia.
- Reduce smoking and alcohol intake: This improves healing and lowers the risk of post-operative complications.
- Ask questions and understand the recovery timeline: Knowing what to expect helps reduce stress and prepares you for a structured rehabilitation program.
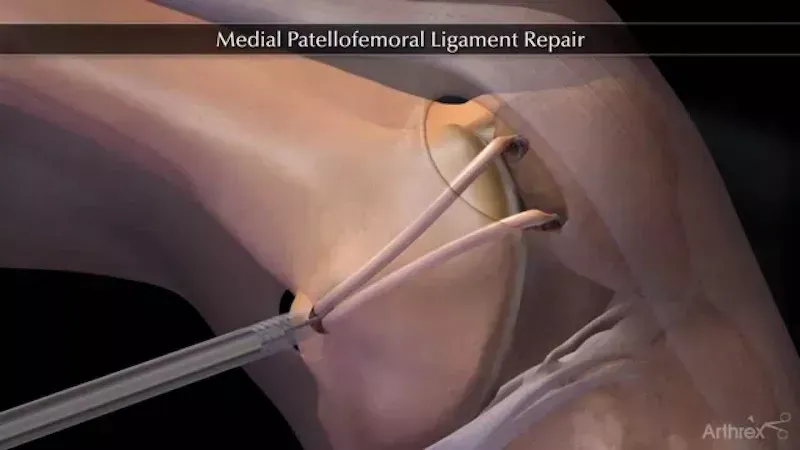
What Happens During an MPFL Reconstruction?
MPFL reconstruction is usually performed under general anaesthesia, meaning you are asleep during the operation. The procedure is typically completed through small incisions, and most patients go home the same day.
During the procedure, several steps take place:
- Anaesthesia and preparation: The leg is cleaned, and a sterile field is set up. Local anaesthetic may also be used to help with pain control.
- Assessment of the kneecap and MPFL: The surgeon may use a small camera (arthroscope) to check the patella, joint surfaces, and surrounding structures.
- Graft harvesting or preparation: If an autograft is used, a small tendon is taken from the hamstring. If a donor graft or synthetic material is used, it is prepared for placement.
- Creation of bone tunnels or anchors: The surgeon makes small channels or uses specialised anchors to secure the graft to the patella and femur in the correct anatomical positions.
- Fixation of the graft: The new ligament is tensioned carefully to restore stability without over-tightening, as the patella must move naturally through its full range of motion.
- Checking patellar tracking: The surgeon moves the knee to ensure the kneecap glides smoothly.
- Closing the incisions: Stitches or medical tape are used, and a compression dressing is applied.
The procedure usually lasts 60–90 minutes, depending on the complexity and whether additional procedures are needed.
What to Expect After an MPFL Reconstruction?
Recovery is gradual and structured to protect the new ligament while restoring strength and flexibility. You may wake up with your leg supported in a brace and experience mild discomfort or swelling, which is normal in the early phase.
Common expectations include:
- Pain and swelling control: Ice, elevation, and prescribed pain relief help manage discomfort.
- Use of crutches: Most patients use crutches for one to two weeks, depending on comfort and surgeon recommendations.
- A knee brace: A stabilising brace may be used to protect the repair while walking and sleeping.
- Physiotherapy: Rehabilitation begins soon after surgery, starting with gentle motion exercises, followed by strengthening, balance training, and functional activities.
- Return to normal activities: Most people return to daily walking within a few weeks. Low-impact exercise often resumes after 6–8 weeks, with sport-specific training beginning around 3–4 months.
- Return to sport: Full competitive sports often require 6–9 months, depending on progress and individual healing rates.
Follow-up appointments allow the surgeon to monitor healing, adjust the brace or exercises, and ensure the graft is functioning well.
MPFL Reconstruction Prognosis
The long-term outlook for MPFL reconstruction is generally very positive. The vast majority of patients regain stability, function, and confidence in their knee. Recurrent dislocation after a well-performed reconstruction is uncommon, and most patients return to the activities they enjoy.
Factors that contribute to excellent results include early physiotherapy, adherence to post-operative guidelines, and correction of any underlying alignment issues. Patients often report improved quality of life, reduced anxiety about their kneecap giving way, and a better ability to participate in sports or physical activity.
Over time, protecting the knee from repeated dislocation also reduces the risk of cartilage damage and patellofemoral arthritis.
MPFL Reconstruction Risks
Like all surgical procedures, MPFL reconstruction carries some risks. Most complications are rare and can usually be managed effectively if they occur. Your surgeon will discuss these with you before surgery.
Possible risks include:
- Infection: Usually prevented with antibiotics and good wound care.
- Bleeding or bruising: Generally settles with time.
- Stiffness or reduced knee motion: Early physiotherapy helps prevent this.
- Over-tightening or under-tightening of the graft: May affect tracking of the kneecap, though modern techniques minimise this risk.
- Graft loosening or stretching over time: Rare when rehabilitation is followed closely.
- Blood clots: Prevented through early mobilisation and, when needed, medication.
- Nerve irritation or numbness: Often temporary.
- Persistent instability: May occur if underlying bone alignment issues are not addressed or if a severe injury occurs after surgery.
Although complications can happen, MPFL reconstruction remains a highly reliable procedure with strong safety outcomes.
What if MPFL Reconstruction is Delayed?
Delaying treatment can have different consequences depending on the severity of the instability and the frequency of dislocations. Some people with mild symptoms may not experience significant progression. However, in many cases, repeated patellar dislocations can gradually damage the joint surfaces.
Possible effects of delaying surgery include:
- Increased risk of future dislocations: The weakened ligament may not heal properly, making the knee more unstable.
- Cartilage damage: Each dislocation can scrape or injure cartilage, leading to long-term pain or patellofemoral arthritis.
- Reduced confidence in knee movement: Patients often avoid certain activities, which may lead to muscle weakness and poorer knee control.
- More complex future treatment: Multiple dislocations or worsening alignment issues may require more extensive surgery later.
Timely assessment and management help protect the knee and improve long-term outcomes.