Shoulder Impingement
What is Shoulder Impingement?
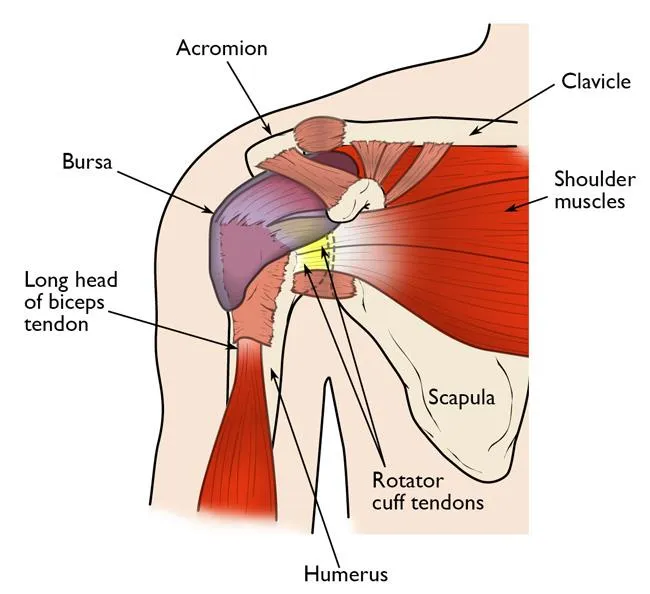
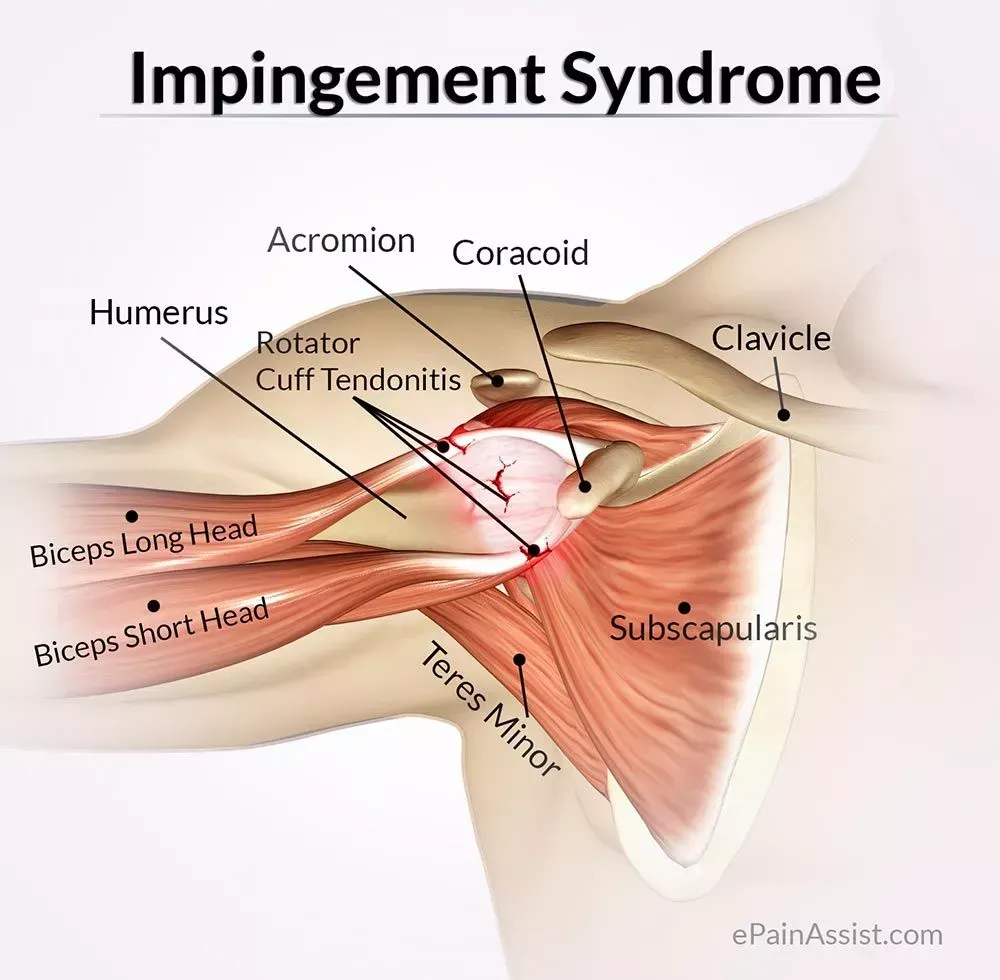
Shoulder impingement occurs when the tendons or the bursa in the shoulder are compressed or pinched by the bones, specifically the acromion (part of the shoulder blade) and the humerus (upper arm bone). This compression leads to inflammation, pain, and a limited range of motion. The condition is most often associated with the rotator cuff tendons and the subacromial bursa, which help stabilise and facilitate shoulder joint movement.
There are two primary joints in the shoulder:
- Acromioclavicular (AC) Joint: Where the clavicle (collarbone) meets the acromion.
- Glenohumeral Joint: Where the head of the humerus fits into the scapula (shoulder blade).
- The rotator cuff—a group of four muscles and their associated tendons—holds the humeral head in place within the glenohumeral joint, enabling smooth movement and stability. When these tendons become irritated due to impingement, it can lead to pain and impaired function.

How Does Shoulder Impingement Impact Your Anatomy and Health?
The tendons in the rotator cuff can become inflamed and swollen, leading to pain and discomfort. This can affect your ability to perform everyday activities, such as lifting objects or reaching for things.
Additionally, if left untreated, shoulder impingement can lead to more severe conditions, such as rotator cuff tears, which can require surgery to repair.
Risk Factors for Shoulder Impingement
Shoulder impingement can affect anyone, but it is more common among athletes who engage in repetitive overhead motions, such as baseball pitchers, swimmers, and tennis players. Additionally, individuals with poor posture or who work in jobs requiring repetitive shoulder movements, such as construction workers or painters, are also at risk.
Causes of Shoulder Impingement
Shoulder Impingement is a common cause of adult shoulder pain. The following are some of the most common causes of shoulder impingement:
- Anatomical factors: Some people may have an anatomical variation, such as a curved or hooked acromion, that can narrow the subacromial space and increase the risk of impingement.
- Overuse: Repetitive overhead activities, such as throwing, swimming, or lifting weights, can cause the rotator cuff tendons to become inflamed and swollen, leading to impingement.
- Poor posture can cause the shoulders to slump forward, reducing the subacromial space and increasing the risk of impingement.
- Muscle imbalances: Weakness or tightness in the muscles surrounding the shoulder can destabilise the joint, increasing the risk of impingement.
- Aging: As we age, the tendons in our shoulders become less flexible and more prone to injury. This can lead to impingement, especially in individuals over 40.
- Trauma: A direct blow to the shoulder or a fall on an outstretched arm can cause impingement.
- Other medical conditions: Certain conditions, such as arthritis, bursitis, and rotator cuff tears, can increase the risk of developing impingement.
Symptoms of Shoulder Impingement
Individuals with shoulder impingement may experience severe pain at rest and during activities, arm weakness, and difficulty raising the hand overhead.
Sufferers of Shoulder Impingement may have the following symptoms
- Minor pain, present with activity and rest
- Pain radiating from the front of the shoulder to the side of the arm
- Pain with lifting and reaching movements
- Pain at night
- Loss of strength and motion
Shoulder Impingement caused by bursitis may include:
- Pain around the outside or tip of the shoulder
- Pain when the shoulder is touched
- Reduced range of movement in the shoulder joint
- Swelling and redness around the shoulder
- Shoulder pain when the arm is raised, such as reaching high shelves or washing hair
The pain may worsen at night, especially when lying on the affected shoulder. It may also worsen after the shoulder is kept still for a while.
The bursa may be infected if the above symptoms are coupled with a fever. This is called septic bursitis, and a doctor should be consulted.
Preventing Shoulder Impingement
Prevention focuses on maintaining strong, flexible, and well-aligned shoulder structures.
- Strengthening exercises: Building rotator cuff and shoulder blade strength improves shoulder mechanics.
- Stretching: Flexibility of the chest, neck, and shoulder muscles helps maintain posture.
- Postural habits: Sitting or standing upright reduces unnecessary strain.
- Balanced training: Avoiding excessive overhead exercises or varying routines can prevent overuse.
- Warm-up before activity: Gentle movement and stretching reduce injury risk.
- Reducing repetitive strain: Taking breaks during physical tasks gives tissues time to recover.
Types of Shoulder Impingement
There are two main types of shoulder impingement: subacromial and internal.
- Subacromial impingement: This is the most common type of shoulder impingement and occurs when the rotator cuff tendons and the subacromial bursa get compressed between the head of the humerus (upper arm bone) and the acromion (a bony projection on the scapula, or shoulder blade). Subacromial impingement can be further classified into three stages:
- Stage I (Edema and Hemorrhage): This stage is characterised by inflammation and swelling of the rotator cuff tendons and bursa, typically occurring in younger patients or athletes.
- Stage II (Fibrosis and Tendinitis): Chronic inflammation leads to fibrosis (thickening) and tendinitis (inflammation) of the rotator cuff tendons, typically affecting patients between the ages of 25 and 40.
- Stage III (Bone Spurs and Tendon Tears): This stage involves the development of bone spurs (osteophytes) on the undersurface of the acromion, which can further compress and irritate the rotator cuff, potentially leading to partial or complete rotator cuff tears. This stage generally affects patients aged 40 or older.
- Internal impingement: This type is less common and occurs primarily in overhead athletes, such as baseball pitchers and swimmers. It happens when the rotator cuff tendons and the labrum (a fibrous rim of cartilage that deepens the shoulder joint) become pinched between the head of the humerus and the glenoid (socket of the shoulder joint) during specific arm movements. This can damage the rotator cuff tendons and the labrum.
Diagnosis of Shoulder Impingement
Consultation
During a consultation, your surgeon will:
- Take a detailed medical history to understand your symptoms, the onset of pain, previous shoulder injuries, and occupation or sports activities that may contribute to the condition.
- Perform a thorough examination of the shoulder, assessing the range of motion, strength, and any areas of tenderness. Specific tests to help diagnose shoulder impingement may include:
- Neer's sign: The surgeon passively elevates the patient's arm, internally rotated, in the scapular plane. Pain during this motion may indicate impingement.
- Hawkins-Kennedy test: The surgeon flexes the patient's shoulder to 90 degrees and then forcefully internally rotates the shoulder. Pain during this maneuver suggests impingement.
- Empty can test (Jobe's test): The patient elevates their arm to 90 degrees in the scapular plane with the thumb pointing downward, and the surgeon applies downward pressure while the patient attempts to maintain their arm position. Pain or weakness during this test may indicate rotator cuff injury or impingement.
- Look for other associated causes of shoulder pain.
Imaging Tests
If the physical examination suggests impingement, the surgeon may order imaging studies to confirm the diagnosis and rule out other potential causes of shoulder pain. Imaging studies can include:
- Ultrasound – This imaging modality can also be used to evaluate the rotator cuff tendons and the subacromial bursa, particularly when an MRI is contraindicated or unavailable.
- X-rays – Since X-rays do not show the soft tissues of your shoulder like the rotator cuff, plain X-rays of a shoulder with rotator cuff pain are usually normal or may show a small bone spur. Occasionally, you can see calcific deposits in the tendon related to calcific tendinopathy. A special X-ray view called an "outlet view" sometimes will show a small bone spur on the front edge of the acromion.


X-rays show the changes to the acromion that narrow the tendon tunnel.
- Magnetic resonance imaging (MRI)
– An MRI can create more detailed images of your shoulder’s soft tissues. If the diagnosis is unclear, it can produce cross-sectional images of internal structures such as the labrum (link back to labral tear), cartilage and rotator cuff.
Arthroscopy
Where appropriate, an arthroscopy may be performed.
Treatment for Shoulder Impingement
The treatment for shoulder impingement typically involves conservative (non-surgical) interventions.
Conservative Treatments
- Rest: Avoiding or modifying activities that cause pain and exacerbate impingement can help reduce inflammation and promote healing.
- Ice and heat therapy: Applying ice packs to the affected shoulder for 15-20 minutes daily can help reduce inflammation and pain. Heat therapy can also help reduce muscle stiffness and improve blood flow to the area.
- Nonsteroidal anti-inflammatory drugs (NSAIDs): Over-the-counter medications like ibuprofen or naproxen can help reduce pain and inflammation.
- Physical therapy: A physiotherapist can design a personalised rehabilitation program to improve the shoulder’s range of motion, flexibility, and muscle strength. This program may include stretching, postural exercises, manual therapy techniques and strengthening.
- Corticosteroid injections: The surgeon may sometimes recommend a corticosteroid injection to reduce inflammation and relieve pain. However, these injections should be used judiciously, as they can weaken the tendons over time.
Surgical Treatments
Surgery may be considered if conservative treatments fail to provide relief or structural abnormalities cause the impingement. Some surgical procedures for shoulder impingement include:
- Subacromial decompression (acromioplasty): This procedure involves removing a small portion of the acromion to create more space for the rotator cuff tendons and reduce impingement. It can be performed using open surgery or arthroscopy (a minimally invasive technique using a small camera and instruments inserted through small incisions).
- Rotator cuff repair: If there is a tear in the rotator cuff tendons, it may be necessary to repair the damaged tissue. This can also be done through open surgery or arthroscopy.
- Bursectomy: In some cases, the inflamed bursa may be removed to reduce pain and inflammation. This can be performed during an acromioplasty.
- Distal clavicle resection: If the impingement is caused by arthritis or bone spurs at the acromioclavicular (AC) joint, a small portion of the distal clavicle may be removed to create more space and reduce impingement.
After surgery, patients typically undergo a rehabilitation program to restore shoulder range of motion, strength, and function.
What if Shoulder Impingement is Untreated?
If left untreated, shoulder impingement can lead to more severe conditions such as rotator cuff tears and frozen shoulder. Rotator cuff tears can lead to significant pain and functional loss. A frozen shoulder is a condition characterised by shoulder stiffness and difficulty with movement, resulting in pain and limited range of motion.