UCL Reconstruction of the Elbow
What is Ulnar Collateral Ligament Reconstruction?
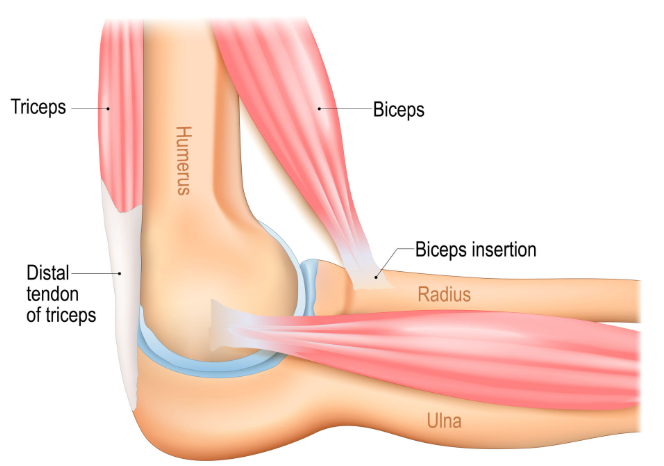
Ulnar collateral ligament (UCL) reconstruction is a surgical procedure used to repair or rebuild the UCL, a key stabilising structure on the inner side of the elbow. This ligament helps control elbow motion, especially during activities that involve strong or repetitive overhead or throwing movements. When it becomes stretched, torn, or completely ruptured, the elbow may feel unstable, weak, or painful during use. Reconstruction is often recommended when the ligament cannot heal on its own or when the injury affects a patient’s ability to perform work, sport, or daily activities without discomfort.
Most patients undergo UCL reconstruction after conservative treatments like rest, physiotherapy, activity modification, and injections have failed to improve symptoms.

Who is Suitable for UCL Reconstruction?
UCL Reconstruction is recommended for individuals with severe UCL injuries, particularly athletes involved in repetitive overhead throwing motions. Here are some indicators that may suggest a patient is suitable for UCL reconstruction:
- A patient with a significant UCL tear or complete rupture
- Athletes who rely on overhead arm motions, such as baseball pitchers, javelin throwers, and tennis players
- Patients experiencing significant functional limitations in activities of daily living, sports, or work due to UCL insufficiency
- Patients who have undergone extensive non-surgical treatments such as physical therapy, rest, and rehabilitation without significantly improving their symptoms

Benefits of UCL Reconstruction
UCL Reconstruction offers several benefits for individuals with significant UCL injuries, including:
- Restores Stability: By repairing or replacing the damaged ligament, the procedure helps stabilise the joint and prevents excessive side-to-side movement during activities that involve throwing or overhead motions.
- Relieves Pain: UCL reconstruction addresses the underlying cause of the pain by repairing the damaged ligament. As healing progresses, many patients experience reduced pain and improved overall comfort.
- Enhances Function and Performance: UCL surgery enables individuals to regain the strength, stability, and range of motion necessary for their specific activities, allowing them to return to their pre-injury level of performance.
- Facilitates Return to Activity: Athletes often seek UCL reconstruction to resume their sports careers after a UCL injury. The procedure and comprehensive rehabilitation program can help individuals safely and effectively return to their desired activity level, including competitive sports.
- Long-Term Results:
UCL reconstruction has shown favourable long-term outcomes for many patients. With proper post-operative care and adherence to rehabilitation protocols, the reconstructed UCL can provide long-lasting stability and support, enabling individuals to continue their chosen activities for years.
Types of UCL Reconstruction
There are two primary types of UCL Reconstruction surgery commonly performed:
- Autograft Reconstruction: Autograft reconstruction uses the patient's tissue to replace the damaged UCL. The most common autograft used is the palmaris longus tendon, typically harvested from the patient's forearm. Sometimes, one of the hamstring tendons, the gracilis, from the patient's leg may be used. Autograft reconstruction is often preferred because it uses tissue from the patient’s own body.
- Allograft Reconstruction: Allograft reconstruction uses donor tissue as the graft material. The donor tissue is typically obtained from a cadaveric source. Allograft reconstruction may be considered when the patient's tissue is unsuitable for grafting or when the surgeon determines it to be the most appropriate option for a particular case. While allograft reconstruction eliminates the need for a second surgical site for graft harvesting, it carries a very low risk of infection transmission.
Both autograft and allograft reconstructions have shown successful outcomes in UCL reconstruction. The choice of graft type depends on several factors, including the patient's overall health and activity level, the surgeon's preference, and the specific characteristics of the UCL injury.
Alternative Options to UCL Reconstruction
Non-Surgical Treatment
Non-surgical treatment options may be explored initially for partial UCL tears or less severe injuries. These include rest, physiotherapy, activity modification, anti-inflammatory medications, and rehabilitation exercises to strengthen the surrounding muscles and improve joint stability.
Regenerative Medicine Therapies
Platelet-rich plasma (PRP) and stem cell injections are regenerative medicine therapies that have gained attention in recent years. These treatments involve using the patient's blood components (PRP) or harvested stem cells to promote healing and tissue regeneration. These can be tried for less severe tears, although outcomes are variable.
Activity Modification
In some cases, modifying activities or adopting different techniques may help individuals manage UCL injuries without surgery. This approach is typically recommended for patients who engage in recreational or non-competitive activities that do not require repetitive overhead motions.
Consulting with an orthopaedic surgeon is crucial to determine the most appropriate treatment plan, whether it involves UCL reconstruction or alternative options.
Preparation Before a UCL Reconstruction Surgery
Before undergoing UCL Reconstruction, several steps are typically taken to ensure the best possible outcome. Here are some common considerations and preparations:
- Schedule a consultation with an orthopaedic surgeon specialising in elbow injuries. During this appointment, the surgeon will evaluate the UCL injury by reviewing your medical history and performing a physical examination. Diagnostic imaging tests such as X-rays, MRI scans, or ultrasounds may be ordered to assess the extent of the damage and aid in surgical planning.
- If UCL reconstruction is deemed necessary, preoperative planning will take place. This involves discussions regarding the surgical procedure, the expected recovery process, potential risks, and anticipated outcomes.
- Before surgery, it is common for patients to engage in a preoperative rehabilitation program. This may involve specific exercises to strengthen the muscles surrounding the elbow joint and improve the range of motion. Preoperative conditioning can optimise surgical outcomes and facilitate postoperative recovery.
- The surgeon will provide detailed instructions on preparing for surgery. This may include fasting guidelines, medications to avoid before surgery, and specific instructions regarding the day of the procedure. It is important to follow these instructions closely to ensure a smooth surgical experience.
What Happens During a UCL Reconstruction Surgery?
Here is a general overview of what happens during a UCL Reconstruction procedure:
- Anaesthesia: The patient will be placed under general anaesthesia, ensuring they are unconscious and pain-free throughout the surgery. Regional anaesthesia techniques, such as a brachial plexus block, may also provide additional pain control during and after the procedure.
- Incision: The surgeon will make an incision over the inner side of the elbow. This incision allows access to the damaged UCL and provides space for surgical instruments.
- UCL Exposure: The surgeon will carefully dissect the layers of tissue to expose the damaged UCL. Special retractors may gently move surrounding structures, allowing clear visualisation of the ligament.
- Ligament Preparation: The damaged portion of the UCL is typically debrided, removing any frayed or torn sections to create a healthy base for reconstruction. When the UCL cannot be repaired, it may be completely removed.
- Graft Harvesting: If an autograft technique is used, the surgeon will harvest a tendon graft from another part of the patient's body. A common graft source is the palmaris longus tendon in the forearm. In some people, the palmaris longus is absent or insufficient. Another common graft source is the gracilis tendon, one of the hamstring tendons in the leg. A pre-prepared donor graft will be used if an allograft technique is chosen.
- Graft Placement: The harvested graft is carefully shaped and sized to meet the specifications for the UCL reconstruction. The graft is threaded through bone tunnels drilled in the ulna and humerus, mimicking the original UCL pathway.
- Graft Fixation: The graft is secured using various fixation methods, such as screws, sutures, or anchors, to ensure stability and promote healing. The specific fixation technique may vary based on the surgeon's preference and the patient's case.
- Closure: The surgeon will close the incision with sutures once the graft is securely fixed. Sterile dressings and a splint are applied.
What to Expect After a UCL Reconstruction Surgery?
Following the surgery, patients will be closely monitored in a recovery area as the anaesthesia wears off. Pain management will be provided to ensure comfort. UCL Reconstruction is usually performed as a day procedure, allowing patients to return home on the same day as the surgery. However, in some cases, an overnight hospital stay may be required for more complex cases or if the surgeon deems it necessary.
UCL Reconstruction Recovery Plan
The recovery plan after UCL Reconstruction is crucial to the overall treatment process. After surgery, your surgeon will provide guidelines based on the type of repair performed and the surgeon’s preference. Common post-operative guidelines include:
- Elevate your arm above heart level to reduce swelling
- Wear an immobilising splint for up to 6 weeks
- Apply ice packs to the surgical area to reduce swelling
- Keep the surgical incision clean and dry
- Physical therapy will be ordered for a range of motion and strengthening exercises. The splint can be taken off to perform the exercises.
- Professional athletes can expect a strenuous strengthening and range-of-motion rehabilitation program for 6-12 months before returning to their sport.
- Eating a healthy diet and not smoking will promote healing
UCL Reconstruction Prognosis
The prognosis for UCL Reconstruction is generally favourable, with many patients experiencing successful outcomes and returning to their desired level of function and activity.
While many patients experience successful outcomes, full recovery and return to pre-injury levels can take time. The healing process and functional recovery are typically gradual, with improvements seen over several months. Close follow-up with the orthopaedic surgeon and physiotherapist, regular progress assessments, and adherence to the recommended postoperative care plan are essential to optimise prognosis and achieve the best possible outcome.
UCL Reconstruction Risks
As with any major surgery, there are potential risks involved. The majority of patients experience no complications following UCL reconstruction surgery; however, complications can occur and include infection, limited range of motion, nerve damage causing numbness, tingling, burning, or loss of feeling in the hand and forearm, cubital tunnel syndrome, and elbow instability.
Remember that the risks and potential complications associated with UCL reconstruction are relatively rare, and many patients experience successful outcomes. Your orthopaedic surgeon will thoroughly discuss these risks with you and provide personalised guidance based on your circumstances.
What if UCL Reconstruction is Delayed?
Delaying UCL reconstruction may allow the UCL injury to worsen. Over time, a damaged UCL may become further weakened or compromised, potentially leading to chronic instability, increased pain, and functional limitations. Over the years, arthritis can develop. It is important to consult with an orthopaedic surgeon as early as possible to determine the appropriate treatment timeline.